Hi, this is Likhith, and today we’re going to talk about kidney and ureteric stones — specifically, how doctors decide whether you need just medicine, or whether you need surgery, and if so, which kind. If you or someone close to you has ever been told “you have a stone,” you’ve probably wondered exactly this. So let’s walk through it together, step by step, in plain language.
Here’s the short version before we dive in: not every stone needs an operation. Some stones can pass out of your body on their own with a little help from medicine. Others are too big, too stuck, or causing too much trouble, and need a procedure to remove or break them up. I’ll take you through each option one at a time, with a picture so you can actually see what’s happening inside.
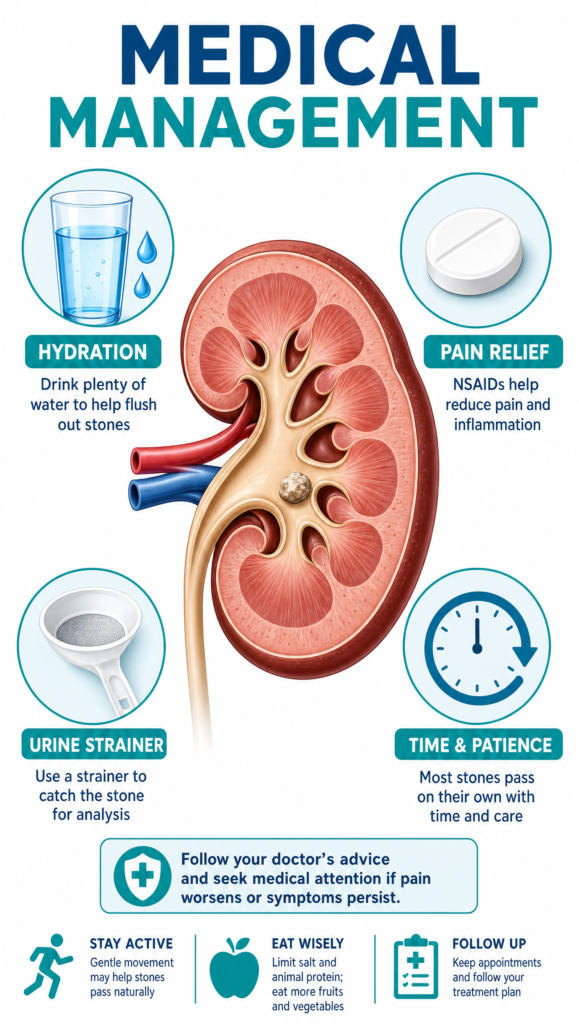
1. Medicine First — Letting the Stone Pass on Its Own
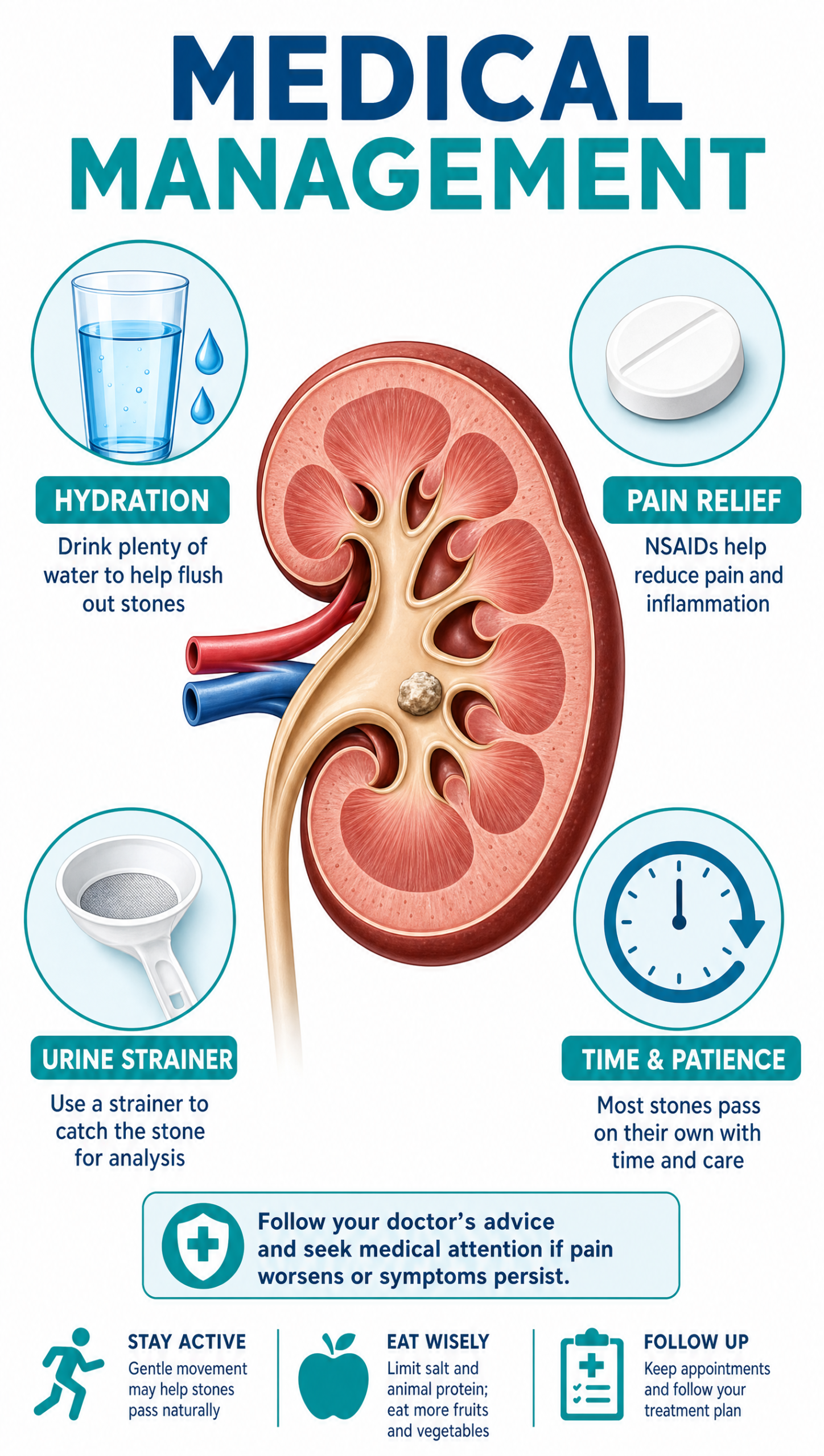
This is simply giving the body time and a little support to pass the stone on its own. The doctor usually prescribes a tablet (often called an “alpha-blocker”) that relaxes the ureter — the tube carrying urine from the kidney to the bladder — making it easier for the stone to slide through. Pain relief and drinking plenty of water are also part of the plan.
Important to understand: none of these medicines actually dissolve or break down the stone itself. Medical management only helps the body push out a stone that’s already small enough to pass — it doesn’t shrink or disintegrate it. There is no medicine or therapy currently recommended by major guidelines that dissolves kidney or ureteric stones; if a stone is too big to pass on its own, a procedure is needed to remove or break it up.
This approach usually works when:
| What doctors check | What’s usually okay |
|---|---|
| Stone size | Small — about 10mm (1cm) or less |
| Infection | None present |
| Kidney working normally | Yes, urine isn’t badly blocked |
| Pain | Manageable with tablets |
| Patience | Willing to wait up to 4–6 weeks |
If the stone still hasn’t passed after that, or if any of these change, it’s time to consider a procedure.
That 4–6 week window isn’t fixed for everyone. It’s a general guideline, not a rule that applies the same way to every patient. How long a doctor is willing to wait depends a lot on whether there’s any infection and how much the stone is blocking urine flow. If there’s even a low-grade infection, or a noticeable degree of obstruction, the doctor may cut the waiting period much shorter — often to just 7–10 days — and move to a procedure sooner. This is because letting a blocked, infected kidney sit untreated for too long raises the risk of lasting damage to the kidney itself.
2. ESWL — Breaking the Stone with Sound Waves from Outside
Now, let’s say medicine alone isn’t going to cut it. The next option, and often the gentlest one, is ESWL.
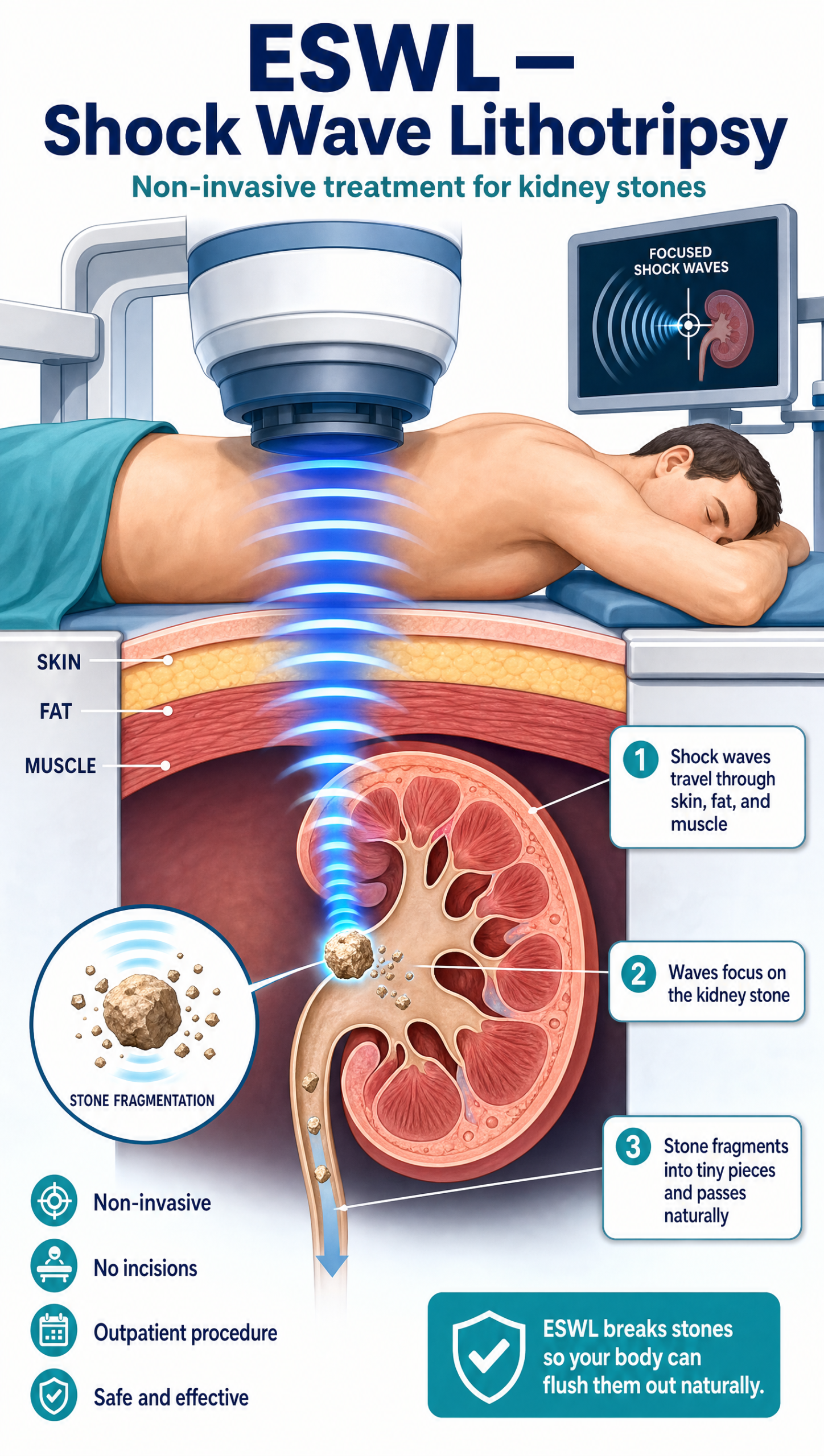
ESWL stands for Extracorporeal Shock Wave Lithotripsy — a long name for a simple idea: a machine outside your body aims focused shock waves through the skin at the stone, breaking it into small, sand-like pieces that then pass out naturally in the urine over the following days or weeks. Before treatment, the doctor first locates the exact position of the stone using either an ultrasound scan (USG) or an X-ray, and the machine is then aimed precisely at that spot.
This is not a surgery. There’s no cut, no incision, and no instrument enters the body at all — the shock waves simply pass through the skin from outside. Because nothing is being cut or inserted, it doesn’t require anaesthesia; most people stay fully awake, sometimes with mild pain relief, and go home the same day.
Good for: smaller stones (up to about 15mm) sitting in a favourable spot in the kidney. It can also be used for stones in the ureter, including the lower part, depending on the stone’s hardness and exact position.
3. RIRS — Reaching the Kidney Stone Through a Thin Scope
If the stone is sitting somewhere ESWL can’t reach well, or it just hasn’t worked, this is usually the next step.
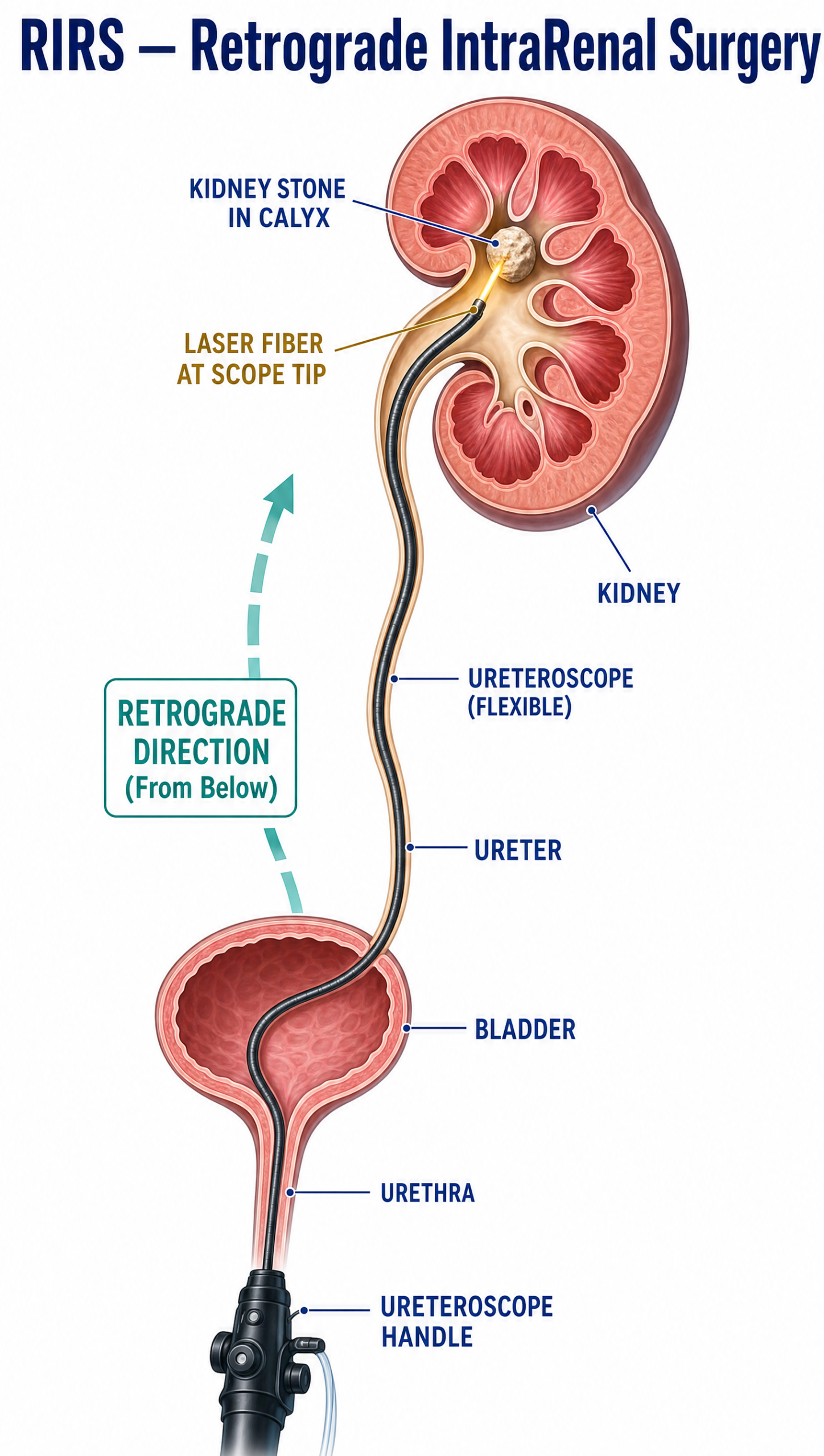
RIRS (Retrograde Intrarenal Surgery) sounds technical, but the idea is straightforward: a thin, flexible telescope is passed in through the natural urine passage — through the urethra, the bladder, and up the ureter — until it reaches the stone inside the kidney. There are no cuts anywhere on the body.
Once inside the kidney, the stone is always broken up using a laser — no other instrument is used here. This is because the flexible scope used in RIRS has a very thin, soft working channel, and a laser fibre is the only tool slim and flexible enough to pass through it and reach the stone. The laser turns the stone into dust or small fragments, which are then removed or left to pass naturally.
Good for: kidney stones up to about 2cm, including ones sitting in awkward spots that shock waves can’t easily reach. Most people go home the same day or the next day.
4. URSL — Removing a Stone Stuck in the Ureter
This one’s for a slightly different situation — when the stone isn’t in the kidney anymore, but stuck on its way down.
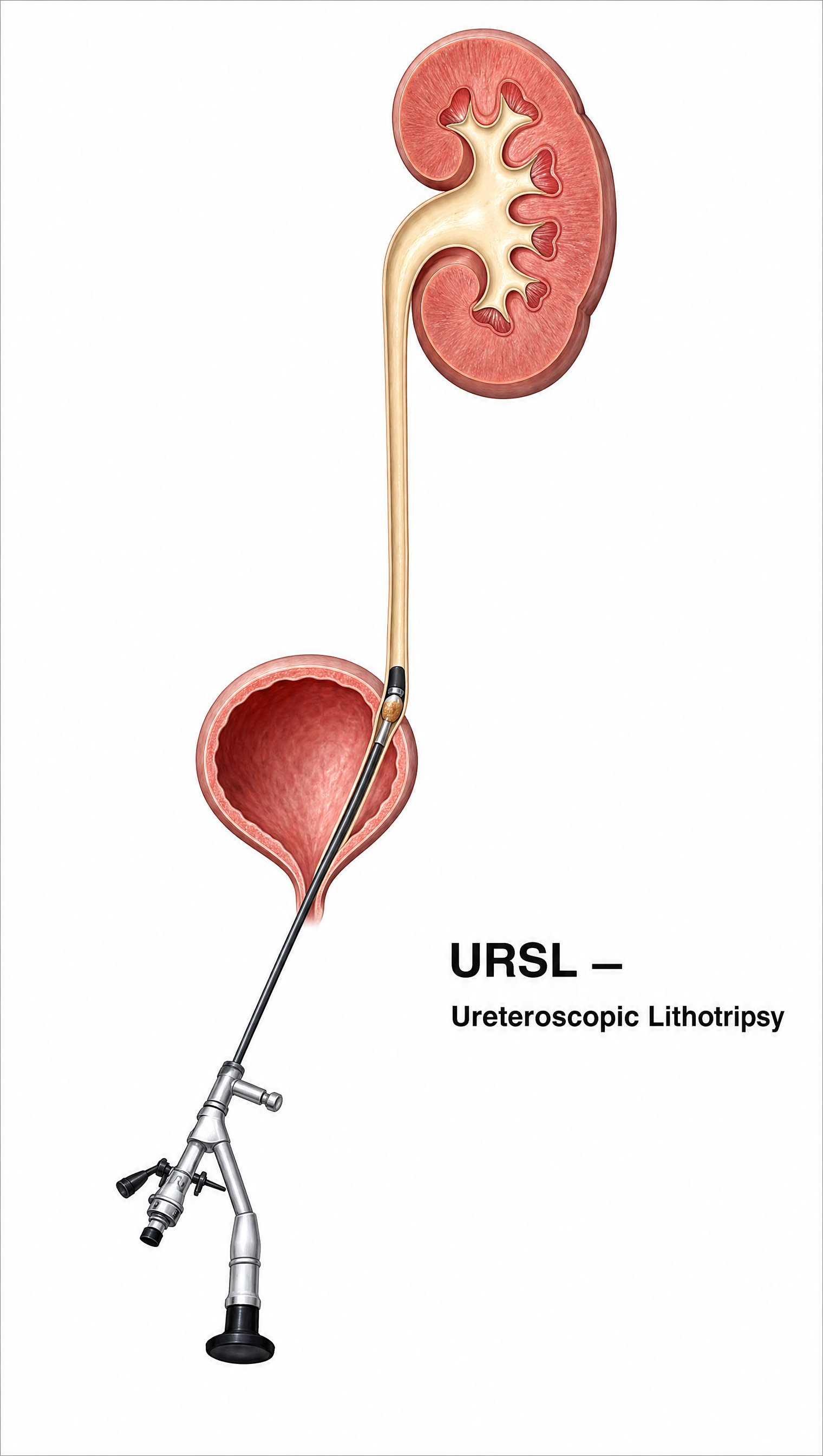
URSL (Ureteroscopic Lithotripsy) is very similar to RIRS, but it treats stones that are stuck in the ureter itself rather than the kidney. A scope is passed up to where the stone is sitting, and the stone is then broken into pieces.
Unlike RIRS, URSL doesn’t always need a laser. Most of the time, the stone is broken using a device called a lithotripter (a pneumatic or ultrasonic probe that taps or vibrates the stone apart) — laser is kept for select situations only. That’s because the ureter is a narrow tube with very little room to spare, and using a laser in such a tight space carries a higher risk of accidentally injuring the ureter wall. A lithotripter is generally considered safer for routine use here, with laser reserved for harder stones or trickier spots where it’s genuinely needed.
Sometimes a small temporary tube (a “stent”) is left in place for a week or two afterward to help the ureter heal and drain properly.
Good for: stones of almost any size that are lodged in the ureter and causing pain or blockage. This is usually the go-to surgical option once medicine alone hasn’t worked.
5. PCNL — A Small Tunnel Directly Into the Kidney
Now we come to the bigger stones — the ones a scope from below just can’t handle efficiently.
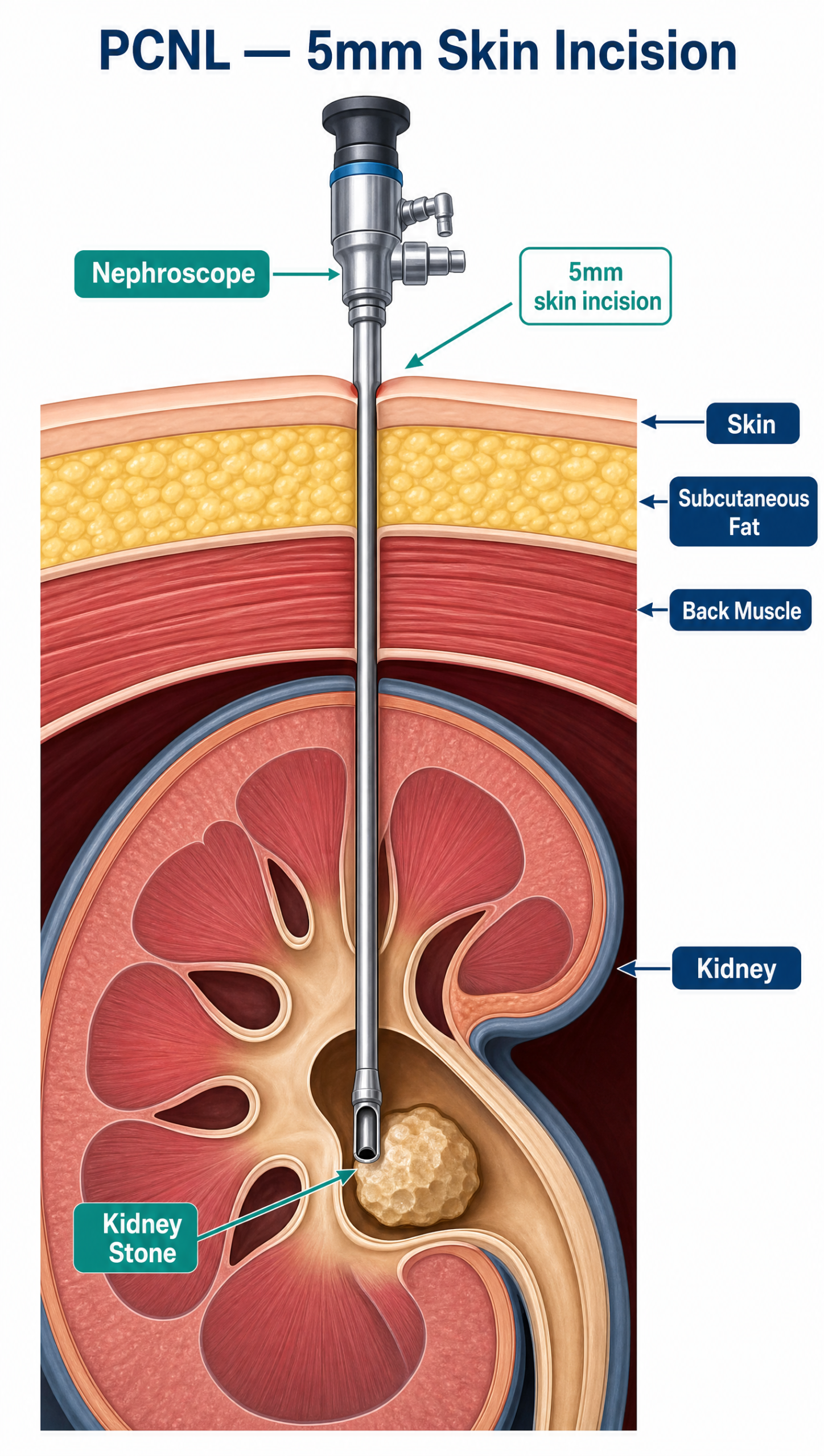
PCNL (Percutaneous Nephrolithotomy) is used for stones too large to clear with a scope from below. Using X-ray or ultrasound to guide them, doctors make a small puncture in the skin of the back and create a narrow tunnel straight into the kidney. A camera and instruments go through this tunnel to break up and remove the stone.
Good for: large stones (2cm or more) and “staghorn” stones, which branch out and fill much of the kidney’s drainage system. It’s more involved than RIRS or URSL but clears big stones in one sitting more reliably.
6. Laparoscopic or Open Surgery — Rarely Needed
And finally, the option you’ll rarely hear about today, because it’s rarely needed.
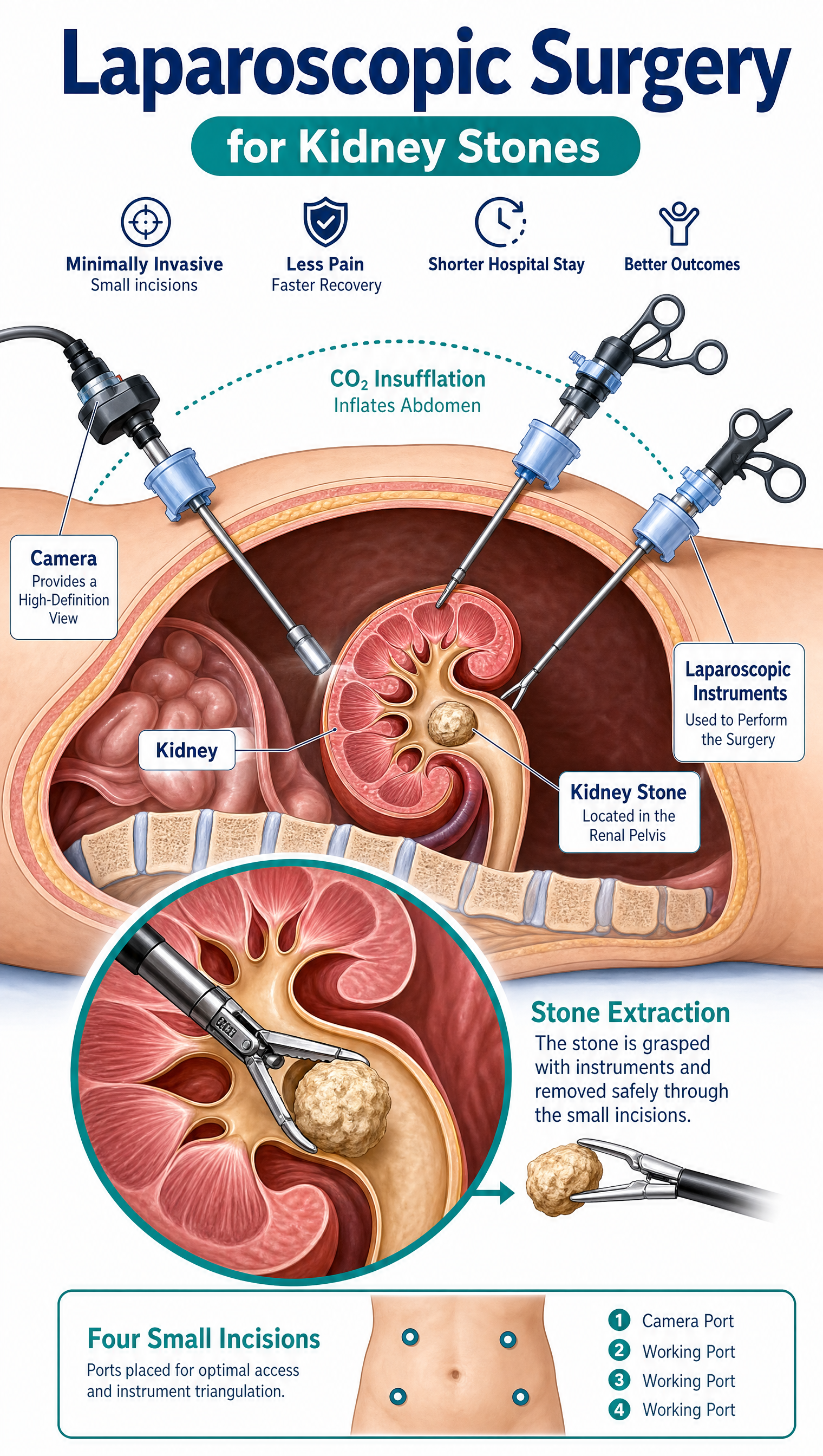
Thanks to the procedures above, full surgery for stones is now uncommon. It’s kept in reserve for unusual situations — very large or oddly shaped stones combined with abnormal kidney anatomy, cases where less invasive attempts have failed, or when another repair to the kidney is needed at the same time. When surgery is needed, doctors prefer a few small cuts (laparoscopic, “keyhole” surgery) over one large incision (open surgery) whenever possible.
Quick Reference
| Type of stone | Usual first choice |
|---|---|
| Small (≤10mm), no infection or blockage | Medicine (let it pass naturally) |
| Kidney stone, under ~2cm, good location | ESWL (sound waves) or RIRS (scope) |
| Stone stuck in the ureter, causing symptoms | URSL (scope to the ureter) |
| Kidney stone 2cm or larger, or staghorn-shaped | PCNL (tunnel into the kidney) |
| Unusual anatomy, or other methods didn’t work | Keyhole or open surgery |
So that’s the full ladder, from a simple tablet and some water all the way up to surgery — and as you can see, most people never need to climb anywhere near the top of it. If you’ve been told you have a stone, the right treatment really comes down to its size, where it’s sitting, and whether it’s causing infection or blockage. Your urologist will walk you through exactly where you fall on this list.
That’s it for this week — thanks for reading, and I’ll see you in the next one.